Health Library
Kuongororwa kweBiopsychosocial: Nei Zvakakosha Mukuronga Kurapa
January 12, 2026
Question on this topic? Get an instant answer from August.
Heino bhuku rebhurogi rawakakumbira.
Chii chinonzi Biopsychosocial Assessment?
Kuongororwa kwebiopsychosocial, kunowanzo kunzi kuongororwa kweBPS, kuongorora kwakakwana kunounganidza ruzivo nezve hupenyu hwemutengi kuburikidza nemaziso matatu akasiyana asi akabatana: biological, psychological, uye social. Chinangwa chayo ndechekuenda kupfuura runyoro rwemarwadzo uye kugadzira kunzwisisa kwe “munhu wese” nezve matambudziko emutengi, kusimba, uye mamiriro ezvinhu.
Funga nezvazvo semuzongoza wechati chemutengi. Nepo mamwe mafomu ekuzvishongedza kwehutano hwepfungwa senge manotsi ekufambira anocherekedza kuchinja kubva musangano kusvika musangano, kuongororwa kweBPS ndiyo mepu yakakwana yakagadzirwa pakutanga kwe rwendo rwepachena.
Iyi nzira yakavakirwa pamuenzaniso webiopsychosocial wakagadzirwa, wakagadzirwa nemudzimai wepfungwa Dr. George Engel muna 1977 source. Engel akataura kuti muenzaniso webiomedical wakapararira waiona hosha sechikonzero chete chemakemikari nemuviri—waive wakamanikana. Akataura kuti kuti unzwisise uye urape munhu chaicho, tinofanira kufunga nezve kubatana kunoita pakati pemuviri wavo (biology), pfungwa dzavo (psychology), uye nyika yavo (social environment). Muenzaniso uyu wakashandura mushonga nehutano hwepfungwa, uchisimbisa kuongororwa kweBPS semuongorori wekuita kwakabudirira.
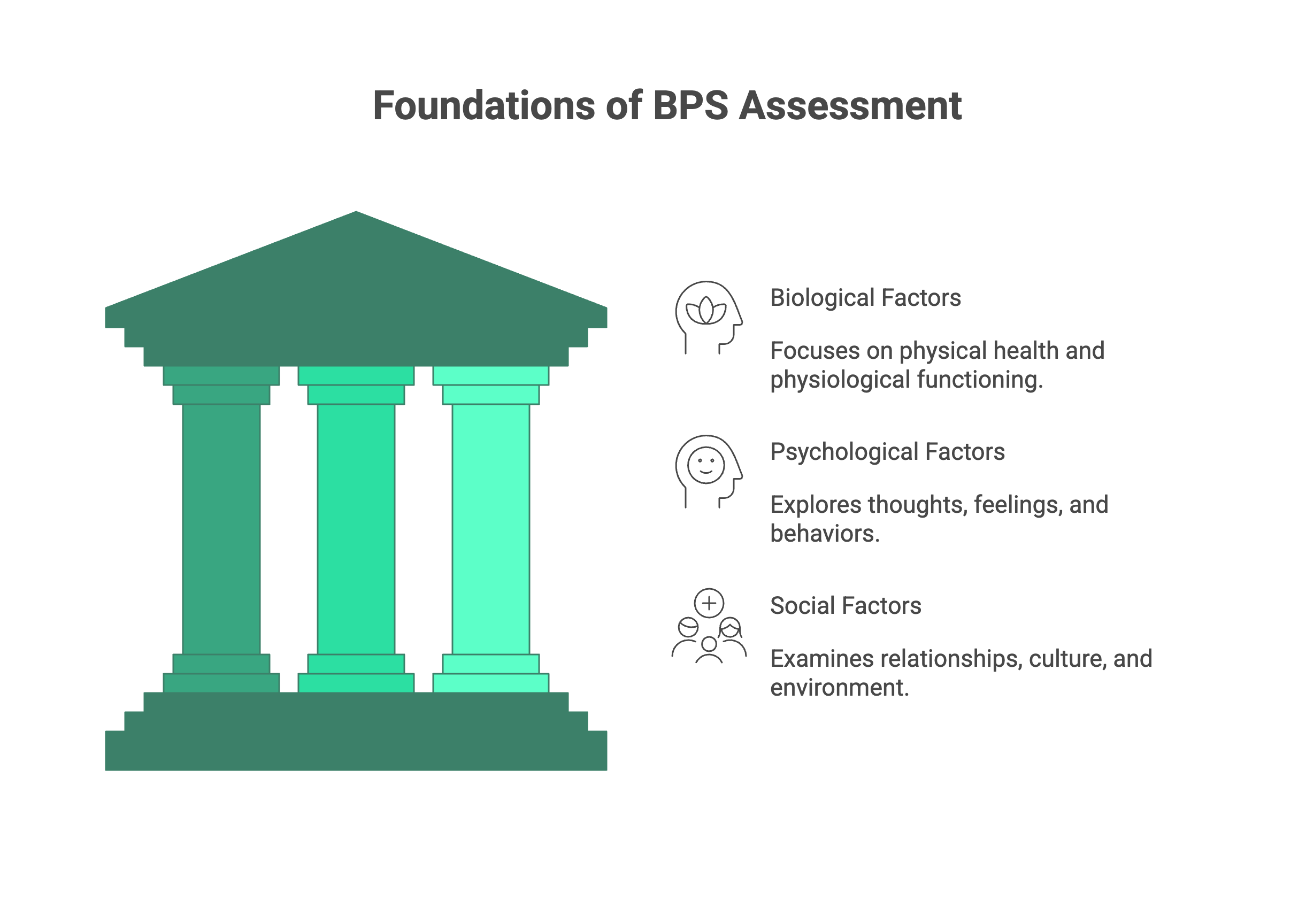
Zvikamu Zvitatu Zvikuru zveBPS Assessment
Simba rekuongororwa kweBPS riri mukuvakwa kwayo kwemapilara matatu. Nekufunda nehutongi nzvimbo imwe neimwe, unovimbisa kuti hapana chakasiyiwa. Ngatibvisei izvi zvinhu zvebiologiki zvepfungwa zvevanhu.
1. Biological Factors (Muviri)
Chikamu ichi chinotarisa kuhutano hwemuviri hwemutengi uye kushanda kwemuviri. Pfungwa nemuviri hazvisi chinhu chakasiyana; kubatana kwavo kwakadzama. Zvichiitika mumuviri zvinokanganisa pfungwa, uye zvakasiyana.
Nharaunda iyi inosanganisira: * Medical History: Zvirwere zvazvino nezvazvino (semuenzaniso, matambudziko ethymuroid, kurwadziwa kusingaperi, chirwere cheshuga), kuvhiyiwa, uye nhoroondo yemhuri yakakosha yemishonga. * Medications: Mishonga yose yakagadzirwa uye isiri yekutenga, zvinowedzera, uye maitiro ekutevedzera. * Substance Use: Nhoroondo uye kushandiswa kwezvino kwedoro, nicotine, caffeine, uye zvinhu zvisiri pamutemo. * Neurodevelopmental History: Chero nhoroondo yekunonoka kwekukura, kuremara kwekudzidza, kana zvirwere senge ADHD kana Autism Spectrum Disorder. * Physiological Basics: Maitiro ekurara (kunaka uye huwandu), kudya uye kudya, uye nhanho yekuita zvemuviri. Pane hukama hwakasimba pakati pehutano hwemudumbu nehutano hwepfungwa, hunowanzo kunzi “gut brain axis” source.
2. Psychological Factors (Pfungwa)
Iyi ndiyo nzvimbo inonyanyozivikanwa kune vanoongorora hutano hwepfungwa. Zvinosanganisira kuongorora pfungwa yemutengi zvakadzama—pfungwa dzavo, manzwiro, maitiro, uye nhoroondo.
Nharaunda iyi inosanganisira: * Presenting Problem: Mashoko emutengi pachavo nezvekuti sei vari kutsvaga kurapwa izvozvi. * Mental Health History: Zvirwere zvapamberi, zviitiko zvapamberi zvekurapa (zvakashanda nezvisina kushanda), uye kugara muchipatara chepfungwa. * Current Symptoms: Kuongorora kwakadzama kwemarwadzo ane chekuita ne manzwiro (kusuwa, kunetseka, kutsamwa), mafungiro (kuramba uchifunga, kuzvidya mwoyo), nemaitiro (kudzivisa, kuzvinetsa). * Risk Assessment: Kuongorora kwakadzama kwezvinofungwa nezve kuzviuraya kana kuuraya, chinangwa, nemaitiro, pamwe chete nemaitiro ekuzvirokana. * Coping Skills: Kuti mutengi anobata sei nekushungurudzika, manzwiro akaoma, nematambudziko azvino. * Cognitive Functioning: Kuongorora kwakajairika kwechirangaridzo, kugona kuisa pfungwa, uye kunzwisisa. * Trauma History: Kuparara kune chero rudzi rwe trauma (kushatiswa, kuregeredzwa, hondo, nezvimwe), kusanganisira hunhu nenguva yezviitiko izvozvo.
3. Social Factors (Mamiriro Ezvinhu)
Hapana munhu anorarama ari ega. Chikamu ichi chinoongorora nyika yekunze inomutsa mutengi, kusanganisira hukama hwavo, tsika, nemamiriro ehupfumi nezvemagariro. Zvinhu izvi zvinogona kuva zviyero zvakasimba zveshungu nerutsigiro.
Nharaunda iyi inosanganisira: * Family and Relationships: Zvinonetsa zvemhuri yekubereka, chimiro chemhuri chezvino, uye kunaka kweukama nevamwe vavo, vana, uye shamwari. * Social Support System: Ndiani wemutengi anotendeukira kwaari kuti awane rutsigiro; manzwiro ekubatanidzwa kana kusurukirwa. * Education and Employment: Zvinyorwa zvedzidzo, nhoroondo yekushanda, kugutsikana pabasa, uye chero kushungurudzika kubasa. * Socioeconomic Status: Kugadzikana kwemari, mamiriro ekugara, uye mukana wezviwanikwa. * Legal History: Chero kupindira kwezvino kana kwapfuura nemumiririri wezvemutemo. * Cultural and Spiritual Factors: Tsika yemutengi, kuzvitsanangura, kutenda kwemweya kana kwechitendero, uye kuti zvinhu izvi zvinokanganisa sei maonero avo enyika nehutano hwavo.
Key Questions to Ask: A Practical Guide for Each Component
Kuziva zvekubvunza ndiko hafu yehondo. Heano mimwe mibvunzo yekuenzanisira yekutungamira kuunganidza kwako ruzivo kune imwe neimwe yemapiyari matatu.
Biological Assessment Questions
- “Ungandiudza nezvehutano hwako hwakazara hwemuviri?”
- “Uri kutora here mishonga yakagadzirwa kana zvimwe zvekutenga?”
- “Pane munhu here mumhuri yenyu ane nhoroondo yemamiriro akakomba emishonga kana hutano hwepfungwa?”
- “Maitiro ekurara ako ungazviotsanangurire sei? Pakatipesarai, maawa mangani ekurara aunowana husiku?”
- “Ndiudze nezvetsika dzekudya dzako pazuva rakajairika.”
- “Mangani nguva dzaunogadzirisa zvemuviri?”
- “Ungatiudza nezve nhoroondo yako nedoro, fodya, kana zvimwe zvinhu?”
Psychological Assessment Questions
- “Nemashoko ako, chii chiri kukuunzira iwe pakurapa panguva ino?”
- “Rini rakatanga kuonekwa nezviratidzo izvi?”
- “Wanga wazotsanangurwa nezve chirwere chepfungwa here kana kuti wakagamuchira kurapa kare? Kana zvakadaro, zvakadini nechiitiko ichocho kwauri?”
- “Paunenge uchinetseka, unozviita sei kuti ubate nazvo?”
- “Wati wati uine pfungwa dzekuti hupenyu haufanire kurarama, kana pfungwa dzekuzviita kana kuita vamwe?” (Tevedzera nekuyerwa kwese kwengozi kana zvichidikanwa).
- “Pane here nhoroondo yekutambudzika, kushatiswa, kana kuregeredzwa kwaunonzwa wakasununguka kugovana nhasi?”
- “Ndezvipi zvimwe zvezvinokudada kwako kana zvinhu zvaunozvirumbidza?”
Social Assessment Questions
- “Ndiani ari akanyanya kukosha muhupenyu hwako zvino?”
- “Ndiani anoita chikamu cheboka rako rekutsigirwa? Ndiani waunotendeukira kwaari paunenge uchinetseka?”
- “Ungandiudza nezvemhuri yako paunenge uchikura?”
- “Mamiriro ako ekugara kwaunoita zvino ungazviotsanangurire sei?”
- “Uri kushanda here kana kuti uri kuchikoro? Zvakadini nechiitiko ichocho kwauri?”
- “Pane here kushushikana kwemari kunokukanganisa zvino?”
- “Une here kutenda kwemweya kana kwechitendero kwakakosha kwauri kana kuti kunobva kune simba?”
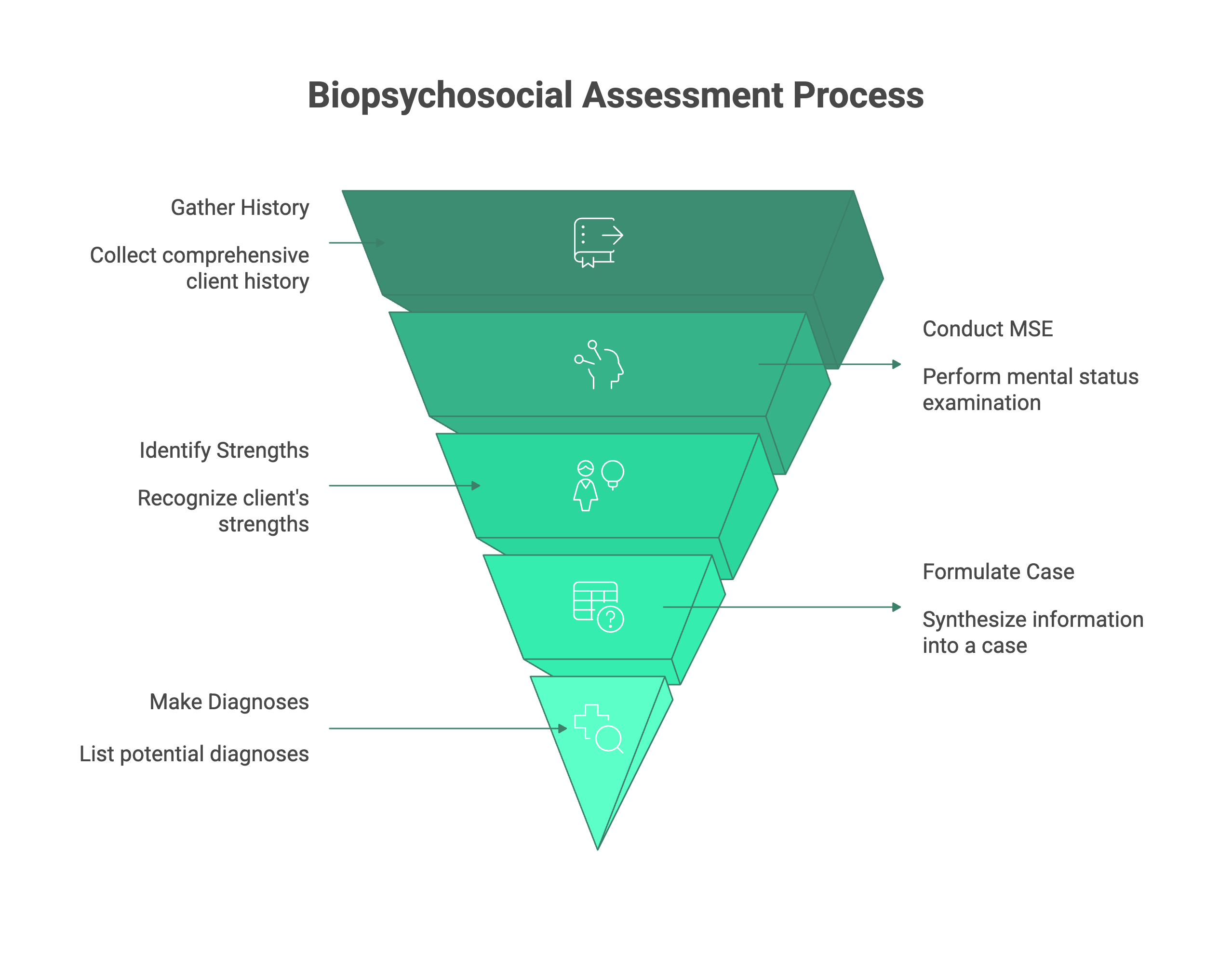
Structuring Your Assessment: The 5 Ps of Case Formulation
Paunenge waunganidza ruzivo urwu rwakawanda, unoita sei kuti ruzvinzwisisike? Pano ndipo panobvakuumbwa kwekesi yeBiopsychosocial. Iri izviro zvekubatanidza data kune nyaya yakabatana inotsanangura mamiriro emutengi wako.
Chimiro chine simba cheizvi ndeye5 Ps yemhando yebiopsychosocial:
- Presenting Problem: Ndeipi chichemo chikuru chemutengi? Nei vachitsvaga rubatsiro zvino? (Semuenzaniso, “Mutengi anoti ari kuona kurwadziswa kwekutya katatu pasvondo.”)
- Predisposing Factors: Ndezvipi zvinhu zvenhoroondo kana zvekumashure zvakaita kuti mutengi ave nedziviriro kune dambudziko iri? (Semuenzaniso, “Nhoroondo yemhuri yekunetseka; nhoroondo yekuregeredzwa kwezvemweya kwehudiki.”)
- Precipitating Factors: Ndezvipi zvinokwezva zvichangobva kuitika kana zvinhu zvakakonzera kutanga kwedambudziko riri kutaurwa? (Semuenzaniso, “Mutengi achangobva kudzingwa pabasa rake.”)
- Perpetuating Factors: Ndezvvi zvinhu zviri kuchengetedza dambudziko uye zvichiita kuti rivepo? (Semuenzaniso, “Mutengi anodzivisa mamiriro ezvinhu evanhu, izvo zvinosimbisa kunetseka kwavo; tsika dzakaipa dzokurara; kusashaya rutsigiro rwevanhu.”)
- Protective Factors: Ndezvipi zvinosimbisa nemidziyo nematsigiro emutengi zvinogona kushandiswa mukurapa? Izvi zvakakosha kune nzira yepasina simba yakavakirwa. (Semuenzaniso, “Mutengi ane chido chekurapa; ane wanano yakagadzikana; anoratidza kunzwisisa kwakanaka.”)
Kushandisa5 Ps yemhando yebiopsychosocial kunoshandura kuongorora kwako kubva pane runyoro rwezviitiko kuita chishandiso chekuongorora chinofambisa chinofambisa chirwere chako nekurongwa kwekurapa.
How to Write a BPS Assessment (Template and Example)
Zvino, ngatitorei kumushandisirwo unoshanda wekugadzira kuongorora kwebiopsychosocial. Chimiro chakajeka ndicho chakakosha. Pazasi pane template yakakwanayekuongorora kwebiopsychosocial yaunogona kushandisa kune yako wega. Kutevera template, uchawana muenzaniso pfupi kuti uone kuti inobatana sei mune fomati yenyaya.
Biopsychosocial Assessment Template
I. Identifying Information * Client Name: * Date of Birth: * Date of Assessment: * Therapist Name:
II. Source and Reason for Referral * Who referred the client? * What was the stated reason for the referral?
III. Presenting Problem * Describe the client’s main concerns in their own words. Include onset, duration, frequency, and severity of symptoms.
IV. History of Presenting Problem * Detailed chronological history of the issues. What were the precipitating events? How has the problem evolved over time?
V. Psychiatric and Mental Health History * Previous diagnoses, past treatment (therapy, medications), hospitalizations.
VI. Substance Use History * Current and past use of alcohol, tobacco, caffeine, illicit drugs. Include age of first use, frequency, and any history of substance abuse treatment.
VII. Medical History * Current and past medical conditions, surgeries, chronic illnesses. Note medications, diet, sleep, and exercise habits. Family medical history.
VIII. Social and Developmental History * Family of Origin: Parents, siblings, childhood environment, history of abuse/neglect. * Education: Highest level achieved, academic performance. * Employment: Current status, job history, satisfaction. * Relationships: Marital status, quality of romantic relationships, children. * Social Support: Friends, community involvement. * Cultural/Spiritual: Cultural identity, spiritual beliefs and practices. * Legal: Any past or current legal issues.
IX. Mental Status Exam (MSE) * Appearance, Behavior, Attitude, Speech, Mood, Affect, Thought Process, Thought Content, Perception, Cognition, Insight, Judgment.
X. Strengths and Protective Factors * Client’s personal strengths, coping skills, supportive relationships, resources.
XI. Clinical Summary and Case Formulation (Using the 5 Ps) * A brief, integrated summary that synthesizes the biological, psychological, and social factors. Use the 5 Ps framework here to structure your analysis.
XII. Diagnostic Impressions (DSM 5 / ICD 10) * List any diagnoses based on the information gathered.
XIII. Treatment Plan Recommendations * Initial goals for therapy, proposed modality (e.g., CBT, psychodynamic), frequency of sessions, and any referrals needed (e.g., for psychiatric evaluation, medical check up).
Biopsychosocial Assessment Example (Brief Narrative)
Client: Jane Doe, 34 year old female.
Presenting Problem: Jane presents for therapy reporting overwhelming anxiety and frequent panic attacks over the past three months, characterized by heart palpitations, shortness of breath, and a fear of “losing control.” She states, “I feel like I’m constantly on edge and can’t relax.”
Summary & Formulation: * Presenting: Generalized anxiety with panic attacks. * Precipitating: Jane was passed over for a major promotion at work three months ago, which she reports felt like a “huge failure.” * Predisposing: Jane has a family history of anxiety (mother and older sister). She describes herself as a “perfectionist” and “high achiever” since childhood, linking her self worth to her professional success. She also has a history of hypothyroidism, which was diagnosed five years ago but has been medically stable. * Perpetuating: Jane’s anxiety is maintained by her long work hours (60+ per week), excessive caffeine intake (4-5 cups of coffee daily), poor sleep (4-5 hours per night), and social withdrawal from friends. She tends to ruminate on work related fears and avoids situations where she might be evaluated. * Protective: Jane is highly insightful and motivated for treatment. She has a strong, supportive relationship with her husband and has successfully used therapy in the past to manage stress during college. She also enjoys running, which she identifies as a positive coping skill she has recently neglected.
This brief biopsychosocial assessment example shows how the information flows into a coherent narrative that points directly toward potential treatment goals, such as developing healthier coping skills, improving sleep hygiene, challenging perfectionistic thought patterns, and reengaging with her social and personal supports.
Common Mistakes to Avoid in Your BPS Assessment
Crafting a high quality BPS assessment is a skill that improves with practice. Here are a few common pitfalls to watch out for:
- The “Problem Only” Focus: It’s easy to get hyper focused on symptoms and deficits. Remember to actively inquire about and document the client’s strengths, resilience, and protective factors. Therapy is about building on what’s strong, not just fixing what’s “wrong.”
- Neglecting a Pillar: Sometimes, a client’s psychological distress is so prominent that we forget to ask detailed questions about their physical health or social environment. A client’s persistent low mood could be linked to an undiagnosed medical condition or profound social isolation. Always give equal weight to the bio, the psycho, and the social.
- Using Clinical Jargon: Write your assessment in clear, objective, and behavioral language. Avoid overly technical terms or acronyms that someone outside your specific modality might not understand. The report should be easily understood by other professionals (with client consent) who may be part of the care team.
- Being Overly Subjective: Stick to the facts. Report what the client says, what you observe, and what collateral information confirms. Differentiate clearly between objective data (e.g., “Client reports sleeping 4 hours per night”) and your clinical interpretation (e.g., “This sleep deprivation is likely exacerbating his anxiety symptoms.”).
conclusion
The biopsychosocial assessment is far more than an administrative hurdle or a piece of paperwork to check off a list. It is a dynamic and collaborative process that honors the complexity of the human experience. It is your first and best tool for building a strong therapeutic alliance, developing an accurate diagnosis, and creating a truly personalized and effective treatment plan.
By investing the time and effort to understand the intricate web of biological psychological social factors that shape a client’s life, you are laying the foundation for meaningful and lasting change. A well crafted BPS assessment is not the end of the intake process it’s the beginning of a successful therapeutic journey.
Health Companion
trusted by
6Mpeople
Get clear medical guidance
on symptoms, medications, and lab reports.

download august