What is the MSE Full Form? A Clinician’s Guide to the Mental Status Examination
By Soumili Pandey
Published on 1/12/2026
Question on this topic? Get an instant answer from August.
What is a Mental Status Examination (MSE)? A Deeper Look
At its core, the Mental Status Examination (sometimes called the mental status exam) is a structured method of observing and describing a patient’s current state of psychological functioning. It involves a systematic collection of data based on the clinician’s direct observations and the patient’s responses to specific questions.
The primary purpose of the MSE in psychiatry and other clinical fields is to gather objective and subjective data to create a comprehensive picture of a patient’s emotional state, cognitive abilities, and thought patterns. This clinical snapshot is crucial for:
- Diagnosis: The findings from an MSE are critical for forming a differential diagnosis for conditions like schizophrenia, major depressive disorder, bipolar disorder, or dementia. source
- Treatment Planning: Understanding a patient’s insight, judgment, and thought content helps tailor therapeutic interventions and medication management.
- Risk Assessment: It is a vital tool for assessing a patient’s risk of harm to themselves or others.
- Monitoring Progress: Repeating the MSE over time allows clinicians to track changes in a patient’s condition and their response to treatment.
Clarification: MSE vs. Mini Mental State Examination (MMSE)
It’s essential to distinguish the MSE from a similar sounding tool: the Mini Mental State Examination (MMSE). While both assess mental functioning, their purpose and scope are different.
- The Mental Status Examination (MSE) is a comprehensive, descriptive, and qualitative assessment that covers a broad range of psychological domains. It is part of nearly every psychiatric evaluation.
- The Mini Mental State Examination (MMSE), on the other hand, is a brief, 30 point, quantitative screening tool used primarily to measure cognitive impairment. It’s often used to screen for and track the severity of dementia. source
Think of it this way: The MSE is like writing a detailed descriptive paragraph about a person’s mental state, while the MMSE is like giving it a numerical score based on a specific set of cognitive tasks.
The 9 Key Components of the MSE: A Comprehensive Guide
To make the MSE easier to remember and perform, clinicians often use mnemonics. A popular one is the ASEPTIC mnemonic (Appearance/Behavior, Speech, Emotion, Perception, Thought Content/Process, Insight/Judgment, Cognition).
Below, we’ll break down the key components of MSE in the order they are often documented, providing a detailed look at what a clinician is observing and assessing.
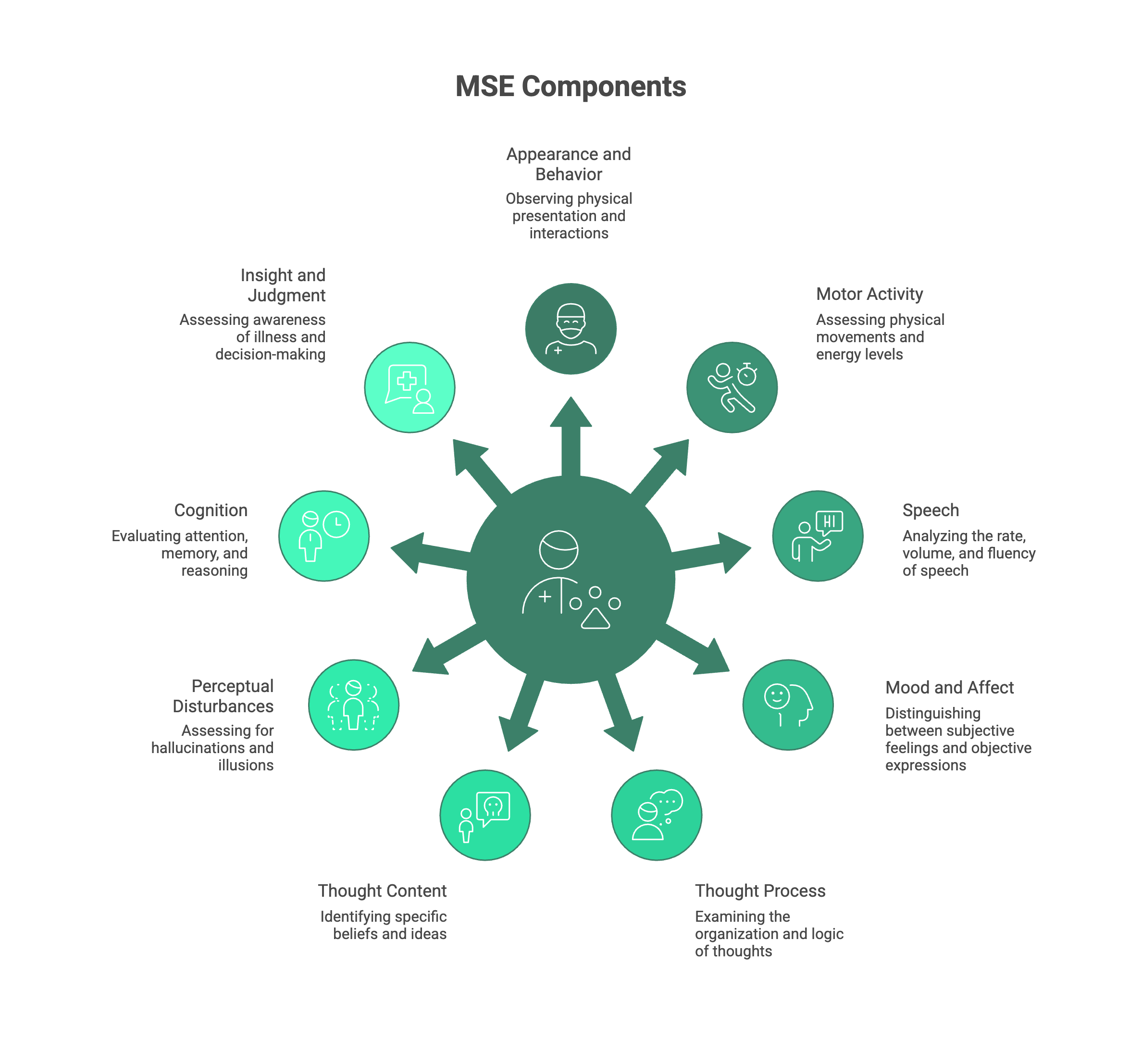
1. Appearance and Behavior
This is the first thing a clinician notices. It’s a general description of how the patient looks and acts during the interview.
- Appearance: How does the patient look? Note their apparent age, grooming, hygiene (e.g., clean, disheveled), dress (e.g., appropriate for the weather, bizarre), and any distinguishing features like scars or tattoos.
- Behavior & Attitude: How are they behaving? Are they cooperative, hostile, guarded, or overly familiar? Note their level of eye contact (e.g., good, poor, piercing) and any unusual mannerisms or gestures.
- A Note on Cultural Considerations: It’s vital to interpret these observations within a cultural context. Norms for dress, eye contact, and personal space vary significantly across cultures, and a clinician must avoid making ethnocentric judgments.
2. Motor Activity
This component focuses on the patient’s physical movements.
- Psychomotor Agitation: Is the patient restless? Are they fidgeting, pacing, or unable to sit still?
- Psychomotor Retardation: Conversely, are their movements slowed down? This can manifest as slowed speech, long pauses, and a general lack of physical energy.
- Abnormal Movements: Note any tremors, tics, lip-smacking, or repetitive movements that might be signs of a neurological issue or side effects of medication.
3. Speech
This isn’t about what the patient says, but how they say it.
- Rate: Is their speech fast and pressured (difficult to interrupt) or slow and hesitant?
- Volume & Tone: Is it loud, quiet, or monotonous? Is the tone angry, sad, or anxious?
- Quantity: Is the patient talkative, or do they only provide one-word answers (poverty of speech)?
- Fluency & Rhythm: Is the speech clear and articulate, or is it slurred or mumbled?
4. Mood and Affect
This is one of the most crucial and often confused parts of the MSE in psychiatry. The key is to remember the difference between subjective and objective.
- Mood: This is the patient’s subjective report of their emotional state. It’s what they tell you they are feeling. You document this using the patient’s own words, such as, “Mood is ‘depressed’” or “Patient reports feeling ‘on top of the world’.”
- Affect: This is the clinician’s objective observation of the patient’s emotional expression, as seen in their face, body language, and voice. Key descriptors include:
- Range: Is the affect full (normal), constricted (limited), blunted (severely limited), or flat (absent)?
- Congruency: Does the affect match the mood? (e.g., A patient smiling while describing deep sadness has an incongruent affect).
- Stability: Is the affect stable or labile (shifting rapidly)?
The distinction between mood vs affect is fundamental. Mood is the climate; affect is the current weather.
5. Thought Process
This component examines the how of a patient’s thinking—the way they organize and express their thoughts.
- Normal: A normal thought process is linear, logical, and goal-directed.
- Disorganized: Common disturbances include:
- Circumstantial: The patient provides excessive, unnecessary detail but eventually gets to the point.
- Tangential: The patient wanders off-topic and never returns to the original point.
- Flight of Ideas: Rapid, continuous speech with abrupt changes from one topic to another, often seen in mania.
- Loose Associations: Thoughts are disconnected, and the logical links between ideas are unclear.
- Thought Blocking: A sudden interruption in thought or speech, where the patient cannot continue their sentence.
6. Thought Content
If thought process is the how, thought content is the what of a patient’s thinking. This is where you assess for potentially dangerous or pathological ideas.
- Delusions: Fixed, false beliefs that are not in keeping with the person’s culture and are held despite evidence to the contrary (e.g., grandiose, paranoid, somatic).
- Obsessions: Recurrent, intrusive, and unwanted thoughts or images that cause significant anxiety.
- Overvalued Ideas: Strongly held beliefs that are not delusional but are given more importance than they should be.
- Suicidal or Homicidal Ideation (SI/HI): This is the most critical part of the assessment. The clinician must ask directly about any thoughts of harming oneself or others, including the plan, intent, and means.
Understanding the difference between thought content vs thought process is key. A patient can have a linear, goal-directed process while describing delusional content.
7. Perceptual Disturbances
This involves assessing for any abnormalities in the five senses.
- Hallucinations: False sensory experiences without an external stimulus. They can be:
- Auditory: Hearing voices or sounds (most common in schizophrenia).
- Visual: Seeing things that aren’t there.
- Olfactory (smell), Gustatory (taste), or Tactile (touch).
- Illusions: Misinterpretations of a real external stimulus (e.g., seeing a coat in a dark room and thinking it’s a person).
- Depersonalization/Derealization: Feelings of detachment from oneself or from reality.
8. Cognition
This is a brief assessment of the patient’s cognitive functions. It is not as in-depth as a full neuropsychological evaluation but provides important clues.
- Level of Consciousness: Is the patient alert, drowsy, or stuporous?
- Orientation: Are they oriented to person, place, and time? (Sometimes “situation” is added as a fourth).
- Attention & Concentration: Can they focus? This can be tested by asking them to spell “WORLD” backward or perform serial 7s (counting down from 100 by 7).
- Memory: Assess both recent memory (e.g., “What did you have for breakfast?”) and remote memory (e.g., “Where were you born?”).
- Abstract Reasoning: Can the patient interpret a proverb like “People in glass houses shouldn’t throw stones”? A concrete interpretation might indicate a thought disorder or cognitive impairment.
9. Insight and Judgment
This final component assesses the patient’s awareness of their situation.
- Insight: Does the patient understand they have an illness and that it requires treatment? Insight can be described as good, partial, or poor.
- Judgment: Is the patient able to make sound, responsible decisions? This is often assessed by asking a hypothetical question, like “What would you do if you found a stamped, addressed envelope on the street?”
Documenting the MSE: A Practical Example
Seeing the theory laid out is one thing; applying it is another. Here is a sample MSE assessment example to illustrate how these components come together in a clinical note.
Hypothetical Patient: John, a 28 year old male presenting to the emergency department with his family due to erratic behavior.
Mental Status Examination
- Appearance and Behavior: John is a 28 year old male who appears his stated age. He is disheveled, with stained clothing and unkempt hair. He is restless in his chair, frequently tapping his foot and wringing his hands. He is intensely focused, with piercing eye contact, and his attitude is irritable and suspicious, though he is minimally cooperative with the exam.
- Motor Activity: Marked psychomotor agitation is present, as evidenced by constant fidgeting and an inability to remain seated for more than a minute. No tics or tremors are noted.
- Speech: Speech is rapid, loud, and pressured. It is difficult to interrupt, and he often speaks over the examiner. The rhythm is fluent, with a tense and angry tone.
- Mood and Affect: Mood is reported as “furious because they are trying to control me.” Affect is labile, full-range, and incongruent with reported mood, shifting from angry glares to inappropriate laughter.
- Thought Process: Thought process demonstrates flight of ideas and tangentiality. He jumps from topic to topic without logical connection (e.g., from discussing the hospital food to a government conspiracy to his plans to become a famous musician).
- Thought Content: Positive for grandiose and paranoid delusions. He believes he has been sent by a “higher power” to “fix the world’s financial system” and that his family is working with the FBI to steal his ideas. He denies suicidal ideation. When asked about homicidal ideation, he states, “I wouldn’t hurt anyone unless they get in my way.” This requires further assessment.
- Perception: Denies visual or tactile hallucinations but endorses auditory hallucinations, stating he hears “the commandants” telling him his mission is important.
- Cognition: Alert and oriented to person and place, but not to time (believes it is 2018). Attention and concentration are poor; he is unable to spell “WORLD” backward or perform serial 7s, stating, “I don’t have time for these stupid games.”
- Insight and Judgment: Insight is absent. He does not believe he has a mental illness and states, “I’m not sick, I’m enlightened.” Judgment is severely impaired, as evidenced by his recent decision to spend his life savings on lottery tickets based on “coded messages” he saw on television.
Other Common Meanings for the MSE Full Form
While the Mental Status Examination is the dominant meaning in clinical practice, it’s helpful to know that “MSE” can stand for other things in different fields to avoid confusion:
- M.S.E.: Master of Science in Engineering
- M.S.E.: Master of Science in Education
So, context is always key!
Conclusion: The MSE as a Cornerstone of Clinical Practice
The answer to “MSE full form” in a clinical context is clear: the Mental Status Examination. More than just an acronym, it is a fundamental and indispensable tool in mental healthcare. It provides the essential framework for a clinician to systematically observe, assess, and document a person’s psychological functioning.
By mastering the components of MSE from appearance and behavior to insight and judgment—students and professionals can develop a keen eye for the subtle and overt signs of mental illness. This structured approach ensures a thorough evaluation, leading to more accurate diagnoses, safer and more effective treatment plans, and ultimately, better outcomes for patients.
For students just learning this skill, the best way to improve is through practice. Start by consciously observing these components in everyday interactions (without diagnosing, of course!). Sharpening your powers of observation is the first step toward mastering this essential clinical art.
Health Companion
trusted by
6Mpeople
Get clear medical guidance
on symptoms, medications, and lab reports.